“Two roads diverged in a wood, and I—
I took the one less traveled by,
And that has made all the difference.” Robert Frost
“Two roads diverged in a wood, and I—
I took the one less traveled by,
And that has made all the difference.” Robert Frost
I received two emails from organizational leadership in the past week that represent milestones to me. One was about our efforts to better manage populations in the context of risk-bearing (pay-for-value) contracts with our payers: “[Partners] is undergoing a planning process to determine what we can do over the next 3 years (2015 to 2017) to better prepare for increased risk in payer contracts….there is a segment of our Hypertension and Diabetes population (and CHF) that would benefit from telemonitoring.” The language here is not dramatic, but the recognition that patient-generated data can be a critical tool for population health management and improved efficiency of care delivery is something we have strived to demonstrate over the last 10 years or more. It feels good to hear it come from others.
The second email came from a senior IT architect: “[The data integration team] are working with the Center for Connected Health to get remote monitoring data into [a scalable, secure database]. From there, the plan is to have the data viewable from, but not necessarily resident in, Epic.” Again, the words are not dramatic in nature, but the recognition, at the highest levels of our IT organization, that it is critical to our future to incorporate patient-integrated data into the care delivery process is a milestone.

I blogged a few months back about how we created the platform referenced in the paragraph above, allowing the easy integration of patient-generated data into our core clinical systems. In fact, we are deliberately using this platform to integrate our Patient-Reported Outcome Measures into the system. This will enable us to bring in both patient self-reported data as well as objective, biometric data and eventually perform analytics on these two data sets.
Partners HealthCare believes that patient-generated data is critical to our future and we’re managing this integration proactively. That does not mean our work is finished. For example, there is currently a significant overhead in managing remote sensors (BP cuffs, scales, etc.) and home hubs (2Net hub, Alere’s Connect device), and getting them back from patients after the program is complete (all of our Connect programs are time-limited). The overhead of purchasing that gear and managing inventory adds cost to the programs and strains ROI calculations.
Why not use what the mobile industry calls BYOD (bring your own device) and software apps on smartphones/tablets? That way, patients who own their own health sensors (so many are available in the consumer space these days) and mobile devices can participate at a much reduced cost to the delivery system.
A recent article in Health Data Management (Providers, Payers Get Appy) sheds some light on what other marquee health care organizations (Kaiser, Geisinger, Children’s Hospital and Aetna were featured) are thinking about the issue of integrating patient-generated data. There are some parallels and some differences to the way we’re approaching it at Partners.
I should caveat the next section of this post by saying that I only read the piece in HDM and did not talk to any of these folks personally. I do know all of these organizations, and have, in the past, spoken with their leadership about their strategies and continue to learn from each other. So I think my analysis is solid. However, I could be wrong.
The biggest difference I see is their belief that patients are already hopping on the bandwagon of buying their own sensors and generating their own data in some sort of massive wave –and that they are all using smartphones and tablets.
As the mHealth field was emerging four to five years ago, I went to conferences and listened to all of the enthusiastic entrepreneurs talk about self-tracking, Quantified Self, consumer enthusiasm for buying health tracking devices, etc. For some time I had a rather unsettled feeling because what I heard in the field did not match our experience at CCH. If we plot degree of illness vs. smart device adoption the graph looks something like this.
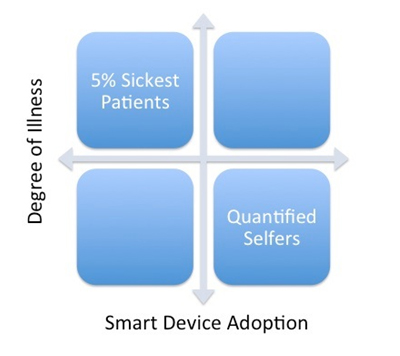
At Partners, the patients we are targeting for connected health programs — to improve care, increase patient self-management and decrease cost — are those sickest five percent — and they are not smart device adopters. The quantified-selfers brimming with smart devices, measuring and monitoring their health and fitness tend not to be folks with chronic illness or patients who drive much utilization of health care dollars.
What the organizations featured in the Health Data Management piece have in common is that they are creating mobile apps/platforms to enable patients who already own smartphones and connected devices to share those data. This approach seems less proactive to me, meaning if you have a smart device and one or more connected sensors and want to share your data with these organizations, they’d be happy to have it. If you do not, they’ll manage you the old-fashioned way with office visits, hospitalizations, etc. The advantage of this strategy, as noted above, is that the cost of technology falls on the patient and the organization rides the adoption curve. However, the adoption of these technologies in sicker patients is still low.
At some point, the five percent of sickest patients will move from the top left quadrant to the top right quadrant in the graphic above. We’ve started to see this with patients asking us for apps, using their own tablets (thank God for Skyping with grandchildren!), etc. But there is almost no penetration of connected sensors in this population yet. We’ve made the commitment at Partners to be more proactive in deploying devices and hubs to these patients. We’re also thinking about how to facilitate adoption of smart devices among these patients — maybe offer coupons to facilitate the purchase of their own scales, BP cuffs, etc.
Then there is the matter of towing the regulatory line. Many of the devices available at Best Buy or the Apple Store are not FDA approved to be used in treating illness. Many of the smartphone apps out there are also not FDA approved. I’m sure this is one reason Kaiser, Geisinger, et al. are creating their own. At least one firm, iHealth, is going in this direction (their platform is FDA approved and available to consumers), and combining their consumer platform into a care delivery process seems like an intriguing option. Qualcomm is offering the 2Net ‘hub’ as a mobile app.
So what are the two roads? One is a proactive approach, using patient-generated data as a core part of population health management and making sure that the sickest patients have the devices to generate objective and self-reported data. The other is perhaps a less aggressive approach, opening the APIs and allowing those with smartphones and connected devices to bring data in. For now, we believe that approach will generate more data from healthy, low-utilization individuals and miss the sickest five percent responsible for 40 to 50 percent of health care costs.
At some point the second path will make the most sense as more, sicker individuals will have smart devices and connected sensors. We’re preparing for that world at Partners.
When do you think it will arrive?





