



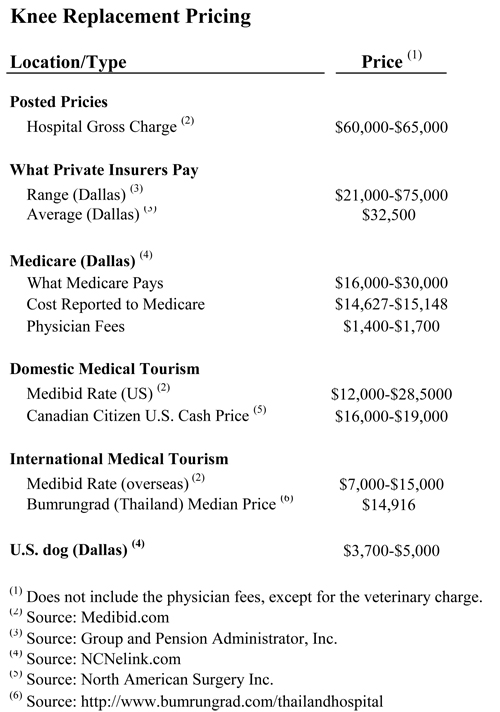
Take a look at the chart below. It shows representative prices for a knee replacement for different patients in different settings. The most shocking thing about the chart is that prices for essentially the same procedure are all over the map. Here are some obvious questions:
Take a look at the chart below. It shows representative prices for a knee replacement for different patients in different settings. The most shocking thing about the chart is that prices for essentially the same procedure are all over the map. Here are some obvious questions:
- Why is the price of a knee replacement for a dog — involving the same technology and the same medical skills that are needed for humans — less than 1/6th the price a typical health insurance company pays for human operations? Why is it less than 1/3 of what hospitals tell Medicare their cost of doing the procedure is?
- How is a Canadian able to come to the United States and get a knee replacement for less than half of what Americans are paying?
- How are Canadians getting knee replacements in the U.S. able to pay only a few thousand dollars more than medical tourists pay in India, Singapore and Thailand — places where the price is supposed to be a fraction of what we typically pay in this country?
- Why do fees U.S. employers and insurance companies are paying vary by a factor of three to one, when foreign, and even some U.S., facilities are offering a same-price-for-all package?
It’s amazing how often people cannot see the forest for the trees. Think how many volumes have been written trying (and failing) to explain why our health care costs are so high. Sometimes the answers to complex questions are more easily found by asking the simplest of questions.

More Read


[But first, a side bar. A study by Miriam Laugesen and Sherry Glied, published in Health Affairs, claims that the reason the U.S. spends more on health care than other countries is the Americans pay higher prices — in particular, higher physician fees. This claim is extraordinary, considering that doctors’ net incomes are only about 10% of health care spending and the amount by which U.S. doctor fees exceed foreign doctor fees is only a couple of percentage points.
Commenting on the study, Uwe Reinhardt says what we have often said: in terms of real resources used, we may not be spending more than other countries. Greg Scandlen is appropriately critical for different reasons. But everyone seems to have missed the far more interesting point: a lot of U.S. patients are not paying more than what foreigners pay.]
Let’s turn to the canine question. When you recover from your knee replacement surgery, let’s say you spend two nights in a hospital room, with all the comforts of a luxury hotel. Fido recovers in a cage, which presumably costs much less. But even with meals, two nights in a hotel should come in under $1,000. The price difference we are trying to explain is about 27 times that amount.
Then, there is the difference in surgeons’ skills. Presumably, the surgeons who operate on humans are more talented, and therefore more valuable. But do you know that an orthopedic surgeon in Dallas typically gets paid an amount equal to about 10% of the $32,500 an insurer pays to the hospital. That’s less than the fee the sales rep gets for selling the artificial knee to the hospital. (I’ll revisit this scandal on another day.)
I suppose you (as a patient) would get more attention than Fido from nurses and support staff for the one or two days of recovery. Guess how much a nurse gets paid in Dallas? It’s about $30 per hour. Steep. But nowhere near the explanation we are searching for.
Let’s take the actual cost hospitals tell Medicare they incur for this procedure. It’s about $15,000, not including surgeon’s fee. But if veterinarians can do it for a third of that amount, it’s hard to see why the human hospital cost isn’t at least half of what it actually is.
The only explanations I can come up with for why human knees cost so much more are (1) government regulations, (2) malpractice liability and (3) the inefficiencies created by the third-party payment system. It looks like these three factors are doubling the cost of U.S. health care.
Let’s take regulations first. In terms of rules, restrictions, and bureaucratic reporting requirements, the health care sector is one of the most regulated industries in our economy. Regulatory requirements intrude in a highly visible way on the activities of the hospital medical staff and affect virtually every aspect of medical practice. In Patient Power, Gerry Musgrave and I described the burdens faced by Scripps Memorial Hospital, a medium sized (250-bed) acute care facility in San Diego, California. Scripps had to answer to 39 governmental bodies and 7 nongovernmental bodies. It periodically filed 65 different reports, about one report for every four beds. In most cases, the reports required were not simple forms that could be completed by a clerk. Often, they were lengthy and complicated, requiring the daily recording of information by highly trained hospital personnel.
Then there is the malpractice system. Estimates place the burden of the system at between 2% and 10% of the cost of U.S. health care. But it’s hard to separate out the effects of malpractice from the effects of regulation. Remember, both institutions are trying to do the same thing: reduce the incidence of adverse medical events (no matter how imperfectly). If a hospital fails to follow a regulation, and that failure leads to a patient death, the failure would undoubtedly be the basis for a malpractice law suit. So the existence of the malpractice system helps encourage compliance with regulations — making them more costly.
Finally, there are the inefficiencies produced by the third-party payment system. We have previously pointed out that when providers do not compete for patients based on price, they typically do not compete on quality either. In the hospital sector, they tend to compete on amenities instead. But the way you compete on amenities is to spend more on amenities. And this adds to costs. To appreciate what your health insurance premiums are buying these days, consider this item from a previous post:
Concierge service. Jacuzzi tubs. Bacon-wrapped scallops or New York strip steak prepared by professionally-trained chefs and brought to your room.
These amenities can be found at most new hospitals in Colorado and across the country. Gone are the days of sterile, white hallways, fluorescent lights and cloth curtains separating patients in the same room. The newest hospitals offer bountiful natural light, warm-colored walls and floors, soothing art and private patient rooms with large windows and relaxation videos.
Sky Ridge Medical Center in Lone Tree features fireplaces on every floor. Children’s Hospital Colorado in Aurora offers video games in patient rooms. The cafeteria at the new $435 million St. Anthony Hospital in Lakewood includes a soda machine that can make 100 different types of drinks.
Now let’s consider medical tourism. If you ask a hospital in your neighborhood to give you a package price on a standard surgical procedure, you will probably be turned down. After the suppression of normal market forces for the better part of a century, hospitals are rarely interested in competing on price for patients they are like to get as customers any way.
A foreign patient is a different matter, however. This is a customer the hospital is not going to get if it doesn’t compete. That’s why a growing number of U.S. hospitals are willing to give transparent, package prices to foreigners; and these prices often are close to the marginal cost of the care they deliver.
North American Surgery has negotiated deep discounts with about two dozen surgery centers, hospitals and clinics across the United States, mainly for Canadians who are unable to get timely care in their own country. The company’s “cash” price for a knee replacement in the United States is $16,000 to $19,000, depending on the facility a patient chooses.
But, and this is what is interesting, the same economic principles that apply to the foreign patient who is willing to travel to the U.S. for surgery also apply to any patient who is willing to travel. That includes U.S. citizens. In other words, you don’t have to be a Canadian to take advantage of North American Surgery’s ability to obtain low-cost package prices. Everyone can do it.
The implications of all this are staggering. Many U.S. hospitals are able to offer traveling patients package prices that are competitive with the prices charged by top-rated medical tourist facilities around the world. (You don’t have to travel to Thailand, after all.) However I would insert this note of caution: Although a hospital with excess capacity gains by charging the marginal customer the marginal cost of care, it may not cover the full costs that must be covered to stay in business if it charges every customer that price. So the prices we are looking at may not be long run equilibrium prices.
The final question is: Why are U.S. employers and insurers over-paying by so much and why does the amount they overpay vary so much?
In part, because in the entire medical marketplace, prices don’t clear markets the way they do in other sectors of the economy. Even MRI’s vary by over 650% in a single town. Furthermore, most providers don’t even know how to price their services because they don’t know what their costs are.
A more basic problem is that insurers are unwilling to adopt what I call the “casualty model” of insurance and what today is more commonly called “value-based purchasing.” Value-based purchasing means that the insurer picks one or more high-quality, low-cost surgical facilities and directs patients to those sites. Patients are free to go elsewhere, but they pay the full marginal cost of those choices when they are exercised. This may include asking the patient to travel.
Being penalized financially for refusing to travel to another city for surgery will not sit well with a lot of employees and their families. But I suspect that this will be only a temporary inconvenience in the evolution of the health care system. Once a few people begin to move to take advantage of lower prices and higher quality, price and quality competition will emerge system wide. At that point the hospital marketplace will begin to resemble a normal market.





{kind=link}