



A recent press release from Health Affairs puts the blame for America’s health care problems squarely on them Greedy Doctors. It says:
A recent press release from Health Affairs puts the blame for America’s health care problems squarely on them Greedy Doctors. It says:
Research appearing in the September issue of Health Affairs shows that physicians in the United States are paid more per service than doctors in other countries–in some cases double. There is also a far bigger gap between fees paid for primary care and fees paid for specialty care in the United States, compared to other countries. These higher fees in turn lead to higher incomes for US physicians than those earned by their foreign counterparts, and are the main driver of higher overall spending in the United States on physicians’ services.
Well, not really. The article, “Higher Fees Paid to US Physicians Drive Higher Spending for Physician Services Compared to Other Countries,” by Miriam Laugesen and Sherry Glied, is a pretty thin reed on which to hang such a sweeping conclusion.
More Read


In fact, the article shows how difficult it is (nearly impossible) to compare service payments between countries, something the authors acknowledge, though they prefer to call it “challenging.”
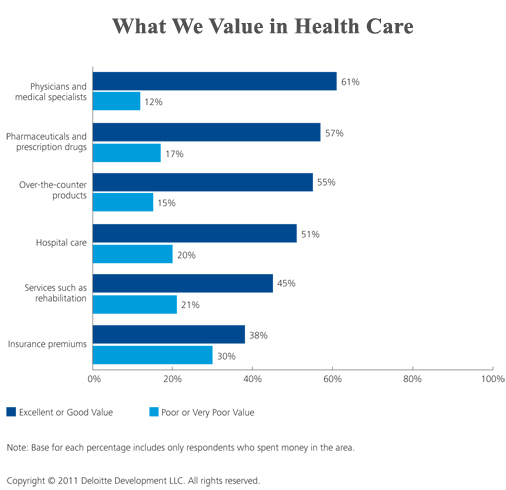
As you’re reading what follows, keep in mind the following chart from Deloitte, which found that the majority of U.S. consumers feel they get their money’s worth in out-of-pocket spending on physician services.

Laugesen and Glied look at primary care and orthopedic surgery (hip replacements) in the U.S., U.K., Australia, Canada, France and Germany, but the payment system is different in each location, and the “service” may be defined differently as well. All of the countries involve a mixture of public and private payments and some have private payers supplementing the public payment. The authors go into great detail about these “challenges,” but still not enough to make sense of it. For instance, surgeons in Germany are salaried, so how do they allocate the cost of a hip replacement against other services? They don’t say. Many of these countries allow physicians to bill on top of the regular payment, but it isn’t clear how much. In the U.S. private payer data on physician payment is proprietary, so the authors rely on HealthGrades reports, which may or may not be reliable.
But the authors satisfy themselves that they have squeezed out enough payment information to write about. Then, to get to “net physician income” they subtract “practice expenses” from the gross. But they don’t have a word to say about what they mean by “practice expenses,” how those expenses may vary between countries, or how they determined how much they cost. Presumably, the expenses will always include rent, utilities, staff salaries, and malpractice insurance costs, but what about physician time devoted to administration? Is that included or not? We don’t have a hint.
The authors take some time to consider educational expenses, which in the U.S. is typically born by the physician, but not so much in other countries, but again this issue is more complicated than the authors are willing to admit. The closest they come is in noting that primary care physicians in the U.S. earn $27,000 more than those on the U.K., which is more than enough to offset the $21,300 annual cost of tuition for the American physician. Well, yes, I suppose it is — assuming everything else is equal, which is a big assumption.
Towards the end of the article, the authors also discuss (a little bit) the fact that higher physician payment in the U.S. may be due to the fact that all professionals in this country command higher wages than in those other countries. Medicine has to compete against business, engineering, law, and other high-earning professions to attract competent people. In one of their tables the authors report on per capita GDP and find the U.S. is much more prosperous than the other countries:

But they don’t try to factor this into their conclusions at all. They might, for instance, have averaged the per capita GDP of the five other countries ($36,685) and found that the U.S. is higher by 28.6%, and used this “relative wealth factor” to adjust their results. But, no, that would not suit the pre-determined narrative of the Health Affairs editors.
Meanwhile, there are plenty of other questions that go unaddressed, including:
- Is the bundle of services the same in each country? What tests are performed during a visit with a primary care physician? Does the surgical fee for hip transplants include follow-up visits or rehabilitation?
- In some countries physicians pay for their health insurance through taxes while in the U.S. they pay with after-tax income. Why not account for that difference in comparing incomes?
- Physicians in the U.S. make much use of Physician Assistants and other “physician extenders.” Is the same true in other countries? If not, don’t American physicians have more unpaid supervisory responsibility than in other countries?
- Similarly, an inordinant amount of physician time in the U.S. is spent on dealing with insurance company paperwork, prior approvals, appeals, and reviews. This time is subtracted from patient care and billable hours. Do other countries have similar issues?
- Finally, a table included in the article shows a wide variation in how health care expenses are allocated in each country:

This table raises all kinds of fascinating questions, such as where does the rest of the money go? Presumably some of it goes to nursing home or dental care, but is it credible that Australia has virtually none of these services?
I don’t know that answers to any of these questions, but these researchers have done us all a disservice by not even asking them or trying an answer them. Sadly, this is another example of “research” that is selected to support a predetermined conclusion.
Is it any wonder that nothing we ever do in health policy actually works?




{kind=link}