Mom had a total knee replacement surgery on Friday, and I’m happy to report she is doing great. She trained for surgery, doing as much pre-surgical physical therapy in the pool and on the bike as her body could tolerate. She is an engaged and determined patient, and she has an engaged family and patient advocate by her side, asking questions she may not know she needs to ask, not being intimately involved in healthcare herself.
Mom had a total knee replacement surgery on Friday, and I’m happy to report she is doing great. She trained for surgery, doing as much pre-surgical physical therapy in the pool and on the bike as her body could tolerate. She is an engaged and determined patient, and she has an engaged family and patient advocate by her side, asking questions she may not know she needs to ask, not being intimately involved in healthcare herself. I’m confident the surgeon was technically skilled, the pain service was attentive and on a schedule for pain management, nurses came in roughly every 4 hours for vitals in the first 48 hours and were kind, always asking her to rate her pain level, and while nutrition services started off like the worst take out order imaginable, they pulled it together over the next couple days. Mom rolled with all of it — no complaints, as she usually does with everything in life.
 As someone intimately involved in the delivery of healthcare, I now understand just how many moving parts are involved in a successful hospital stay, and I am also more critical of the care being delivered. I also know it is the greatest gift to care for patients in their time of need, and that as we do this, we are also delivering a costly service that the patient is paying for–one way or another. As such, we need to step up and design and deliver care that addresses the patient’s needs, values, preferences and goals from the outset. While the flow of Mom’s care seemed to even out nicely over the course of her stay, and on a weekend no less, I still saw a number of ways that care could have been more patient-centered. Here are a few:
As someone intimately involved in the delivery of healthcare, I now understand just how many moving parts are involved in a successful hospital stay, and I am also more critical of the care being delivered. I also know it is the greatest gift to care for patients in their time of need, and that as we do this, we are also delivering a costly service that the patient is paying for–one way or another. As such, we need to step up and design and deliver care that addresses the patient’s needs, values, preferences and goals from the outset. While the flow of Mom’s care seemed to even out nicely over the course of her stay, and on a weekend no less, I still saw a number of ways that care could have been more patient-centered. Here are a few:
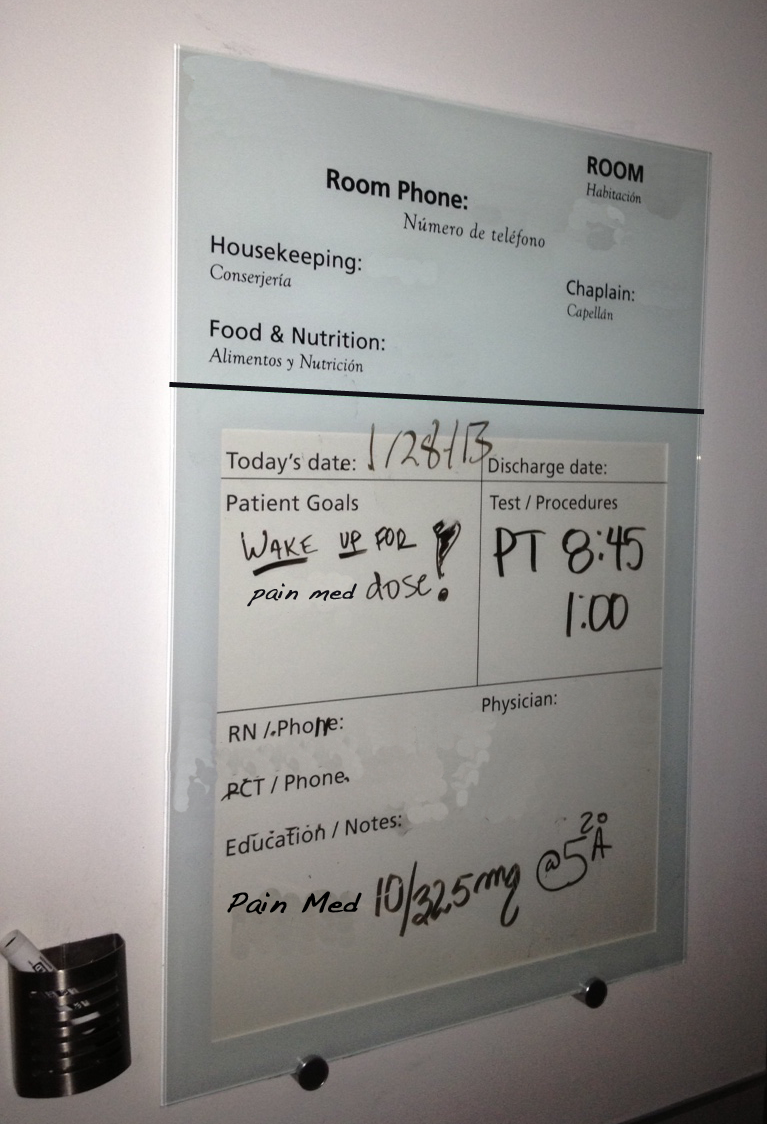
- The white board in the room had a place for Patient Goals but those were never addressed until I wrote her wishes to be woken up for pain medication on the board.
- Each member of the care team came in separately–the patient or family was not included in a meaningful way in any of the rounds or handoffs.
- The surgeon only did surgeries on Fridays–a nightmare for anyone savvy to the potential hazards of night and weekend care in hospitals.
- Mom was being given instructions while on narcotic pain medication, fresh out of surgery and over the course of the next two days.
- We had to ask the questions, and were not invited into the conversation in a meaningful way as part of the care team.
So the first procedure-related hurdles appear to have been cleared. She’s alive and well, and heading home today. As I remain mindful of the potential for an infection lurking beneath her bandage, or a fall once she’s home, she remains positive and upbeat, ready to do the other knee next year. She has had a positive experience of care, and reports feeling very informed about her procedure and what is to follow, and I’m grateful for the care she received. I can’t help but wonder, however, about the other patients I saw with similar bandages, who may not have been referred to their surgeon by one of his own work colleagues, or did not have a cadre of family and extra ears present to listen in as the pain medication kept them comfortable–I hope their experience was equally as positive. It also reminded me just how resilient we are all are–that despite care not quite as patient-centered as I might have liked, Mom is happy and so far, healing nicely.

First Posted on Educate the Young



