With President Obama’s second inaugural speech calling for a reduction in rising healthcare costs, the need for reassessment of health and social service delivery in the physician’s office, medical homes, accountable care organizations, urgent care/retail center, community clinics, hospital, health system and COMMUNITY ring louder. For the good news, With President Obama’s second inaugural speech calling for a reduction in rising healthcare costs, the need for reassessment of health and social service delivery in the physician’s office, medical homes, accountable care organizations, urgent care/retail center, community clinics, hospital, health system and COMMUNITY ring louder. For the good news, the Journal of American Medical Association recently published a study demonstrating that quality improvements within the community helped reduce hospitalizations and readmissions for the Medicare population.
With the help of CMS funded Quality Improvement Organizations (QIO), community wide interventions were coordinated between hospitals, nursing homes, home health agencies, physicians, hospice organizations and senior centers, resulting in roughly 5.7% reduction in hospitalizations and readmissions for fourteen diverse areas.
And while it is critically important to continue the investigation and sharing of best practices for hospitalization and readmission reduction, I was also intrigued by Ted Eytan’s recent post, Pioneering Idea: Your Patient’s Community Health Needs Assessment on the Desktop. Reminiscing about his ‘community oriented primary care’ instruction in medical school, he introduces a new community health assessment platform available online at http://www.chna.org along with his thoughts about how to utilize it. As a futurist, he suggests that information could be integrated into a patient’s medical record for analysis and discussion.
With ten Community Oriented Primary Care Centers currently administered by Parkland Health & Hospital System, I began to wonder if having this type of data available for patient discussion would be beneficial? Already fluent in patient registries and predictive analytics for increased prevention and better outcomes, this sounds like the perfect storm for the Parkland Center for Clinical Innovation.
And for those remaining physician practices, accountable care organizations, medical homes, hospitals and healthcare networks delivering healthcare on a daily basis, could this information be made available to patient and provider alike on one’s website, app, iTriage – or better yet, a game created to crowdsource ideas for improving community status?
As Ted aptly puts it, morphing from a health advocate to a “health activist” requires innovative ideas like the one above in order to, one day, become part of a human development system, designed to help all people achieve their life goals through optimal health of the individual, family, community and society.
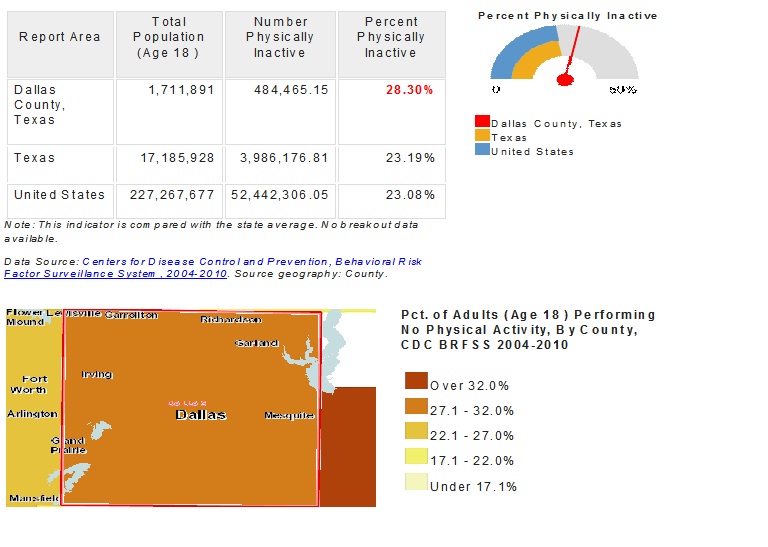
Physical Inactivity (Adult)
This indicator reports the percentage of adults aged 18 and older who self-report no leisure time for activity, based on the question: “During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?”. This indicator is relevant because current behaviors are determinants of future health and this indicator may illustrate a cause of significant health issues, such as obesity and poor cardiovascular health.