





Ebola — this word has its own hashtag, millions of tweets, hundreds if not thousands of articles in the past month, and the power to frighten many people. Fear is playing a large role in how this disease is perceived, which is a poor foundation for managing its spread.
Ebola — this word has its own hashtag, millions of tweets, hundreds if not thousands of articles in the past month, and the power to frighten many people. Fear is playing a large role in how this disease is perceived, which is a poor foundation for managing its spread.
Communicating Key Information
Electronic health records (EHR) are essential tools in clinical care. When written words in an electronic record become the primary way information is shared among busy clinical staff, I believe we inject increased risk into clinical care.
The nation is following the Dallas case almost minute by minute but let’s not lose sight of a crucial lesson from the first day: the role played by the EHR. Critical information was entered but not used for clinical decision-making. Important information about travel outside of the US was correctly entered into the EHR but in a section not viewed by all members of the clinical team. To avoid a repeat of this tragic misstep in Mr. Duncan’s care the check-list for travel outside the US is now in a prominent location.
This change in the EHR may be helpful, but used alone it is a reactive approach that misses the crucial lesson. Where is the “safety huddle” when a red flag emerges on initial assessment?
I recall reading a post in Health Leaders Media that received many comments from nurses about doctors not reading nurses notes. I have a long time bias that the patient’s notes should be interdisciplinary. I also recognize that this is an uphill battle, given many of the EHRs are not designed around teamwork. We can make team communication a priority by learning from this tragedy.
Crucial Lesson: Basics Matter
The importance of direct conversation with key members of the care team cannot be overstated. A red flag that arises on a patient assessment or condition requires more than a note in the electronic record! There are various strategies being used to communicate concern, such as clinical huddles, SBAR and others but the process of talking to one another is at the core.
Our communication cultures must improve, and quickly.
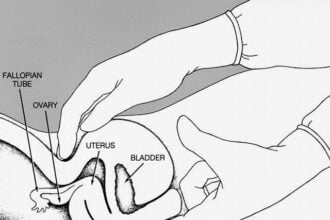
If the Dallas case is an overall call to immediate action to avoid infection risk, then we are long overdue for a fundamental shift to the basics. Let’s remind ourselves that healthcare-associated infections (HAI) in general remain in need of practice changes. Catheter-Associated Urinary Tract Infections (CAUTI) account for more than 30% of those infections, about 200,000 people a year. Often this is the result of inappropriate placement or forgetting to remove the catheter in <48hours when the clinical condition does not warrant it remaining in the patient’s bladder.
RELATED CONTENT: CMS Requirements Will Be “Trick” for Hospital Budgets this October
Clinicians understand the need for clear and accurate information sharing. They also feel the dissonance when they do not have the time to actively listen to a patient or coordinate with other members of the team for patient needs.
What lessons do you believe we can take away from the Dallas case to improve care in your area of practice?
ebola / shutterstock




{kind=link}
{kind=link}