




Summary: A friend told us the other day that the all payer claims database, also known as an APCD, is the answer to health cost transparency. By collecting the payment info together where it can be compared, by this logic, the secrecy in the system will be erased. We said, not so much. Why? Here are some reasons.
The idea of the all-payer claims database is fairly simple: all payers will contribute their payment information to a central database. This means that Blue Cross and Humana and Aetna put their information in, as will the government (it’s a huge payer under Medicare for the elderly, Medicaid for poor and disabled people, and TriCare, for the military).
More Read


Then the central authority — usually a state agency, or a nonprofit with state agency money — can assess, gatekeep, sanitize data, protect access and the like. Providers, payers and provider networks are also essentially then able to gain access to this data under certain rules, which vary by state.
“APCDs are large-scale databases that systematically collect medical claims, pharmacy claims, dental claims (typically, but not always), and eligibility and provider files from private and public payers. The first statewide APCD system was established in Maine in 2003,” according to an issues brief from January 2014 by the national APCD council. “By 2008, five states (Kansas, Maine, Maryland, Massachusetts, and New Hampshire) had passed legislation and established APCDs.”
What the data is used for is another thing.
Rules for collecting and maintaining data vary from state to state; rules for access to the data also vary. And then, if you have access to the data, meeting whatever criteria are established, you need to have big data munging capabilities to take advantage of it, which we happen to know are in short supply.
As an individual, you don’t have access to what’s in the APCD about you, or generally about providers.
So what’s the point? Once all claims and payments are put together, the theory goes, comparisons will be possible and costs will — must — go down. The payers, whose claims payment information has been secret, will suddenly be out in the open, or at least in a place where their company’s data can be compared with others’ data.
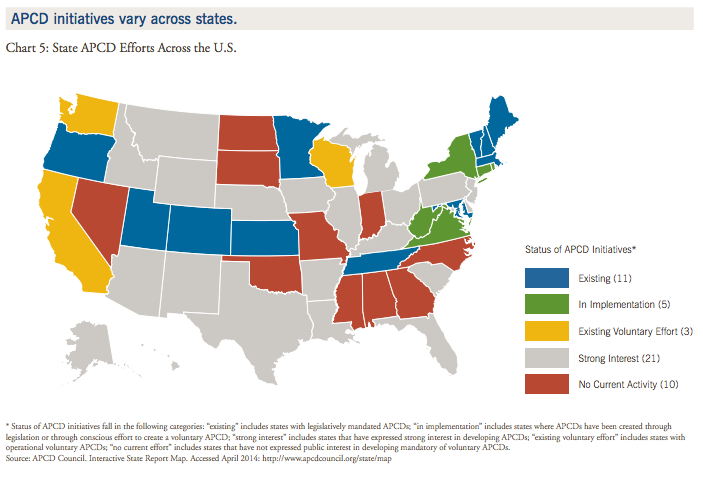
This is a huge generalization, but generally we see three broad types of APCD status among the states:
- States that have one and make it accessible, but not to consumers, and with widely varying criteria and degrees of usefulness.
- States that have one and make tools from it that are helpful to individuals (Colorado, Maine, New Hampshire and Texas have tools that are useful).
- States that don’t have an APCD.
Not everyone’s enthusiastic about the APCD
We have heard from some APCD owners that this phenomenon will be the solution to all health care woes. On the other hand, some scoff at the idea that an APCD will solve anything.
The fairly new nonprofit Catalyst for Payment Reform, in fact, issues its own transparency grades, state by state, and it seems to think that an APCD by itself is not a special sign of goodness. Here’s a blog post by its executive director, Suzanne DelBanco, on state transparency measures.
What have the effects of APCD’s been on reducing costs? So far, one thing is clear: Massachusetts has an APCD and it still has the highest or nearly the highest per-capita medical spending in the nation. So an APCD does not automatically bring down costs, unless it can be proven that Massachusetts’ costs would have gone up even further without the APCD, and we have seen nothing of the sort.
Further, if the data is available only to industry, and not to individuals, then the information is locked away from any place where we could use it in decision-making.
Why haven’t we at clearhealthcosts.com asked for APCD access? The databases run state to state, and so far none of our states of intense focus have one. Also, they vary greatly by contents, value, access restrictions and the like.
Adrian Gropper, an M.D. and privacy/open data advocate in Massachusetts, wrote in a recent blog post about the state’s APCD, “Your information can be used by business to manipulate prices for maximum profit, or by you to inform your choice of health insurance plans and health care providers. Unfortunately, business can get your information but you can’t. ”
One other point: the idea of making such a database seems to be a good one, but if the information is collected and then locked away from individuals where it can be used to make decisions, and rather kept in a data silo where real people can’t get at it, does that just add a level of intermediation? Does it just create another database where information is hidden? And what portion of the transparency movement’s energy and mindshare is spent on legislation, regulation and management of the APCD, without delivering useful consumer tools?
We are always looking for ways to help consumers and so far the APCD movement doesn’t seem to have been much help.
The state of play with APCD development
“Before the Affordable Care Act was passed and signed into law in 2010, only a few states had APCDs, such as Maine, Maryland, Massachusetts, and New Hampshire,” the Association of Health Care Journalists reported. “Since the act was passed, 19 states have APCDs in varying stages of development and at least 21 states are considering laws to create them, the APCD Council reported in June 2014.”
One of my favorite research resources is the National Council of State Legislatures. They are in touch with statehouses nationwide, and they wrote this report about the state of play in the APCD world.
So here’s a Robert Wood Johnson paper describing the state of play on the APCD front in late 2013. Their conclusion on the state of the art: “It is too early to determine whether all-payer claims databases can help states control costs.”
Some might say the APCD movement is good, but is not revealing but rather obscuring the real consumer-provider economics — the exchange of value between the provider and consumer of the service. In other words, it’s adding another level of intermediation in a marketplace that’s already heavy with intermediaries.
We were approached by a state APCD official who said he’d love to join hands with us and create a joint project, a version of PriceCheck, our crowdsourcing tool, in conjunction with his data. Our data on pricing, delivered by our reporters and by consumers, could then be compared with the pricing data delivered by payers, serving as a corroboration or a challenge of the validity of the data — and presenting a 360-degree view of pricing.
We talked about the possibility, and he then suggested that he’d raise it with his board members, who include insurers, providers, brokers and others. He said he expected that they’d resist, and indeed he did not call back.
A look at Colorado’s APCD
Colorado has one, and has used it to make this consumer-friendly tool to let people shop for procedures — for now, only maternity care, hip and knee replacements.
Even a limited data set can be useful — anything that helps people orient themselves in the marketplace. So, could I go there and price a hip replacement? Here’s what the site says.
“What can I expect to actually pay?
“A: Actual prices for services may differ substantially depending on your specific health insurance benefit package, whether the provider/hospital is in your health insurance network, your current health status, and any complications or confounding health factors you may have. To assist you with determining your costs, a cost calculator (click on ‘My Price’) is available on the website that helps factor in your co-pays and deductibles. For more specific information on the price you might expect to pay, contact your health insurance company.”
I’ve asked the Colorado folks to explain what their plans are for next steps, and also who their major customers are. I’ll update when they reply.
Pennsylvania also has an APCD. I’ve asked them for information about who’s using their data and what for, and I’ll update when they reply.
A look at the Massachusetts APCD
Massachusetts has one, for example, run by the Center for Health Information and Analysis (CHIA! another acronym!).
Here’s how it’s described on the site: “While several states have All Payer Claims Databases, the MA APCD has a unique focus on the efficiencies to be achieved by having one state agency collect and aggregate data from payers. CHIA offers the additional benefit of having the infrastructure to monitor and work with the payers to improve data quality and completeness.”
As noted, Massachusetts has either the highest or second highest health care costs per capita in the nation.
Massachusetts makes its data availably only via an application process: “MA APCD data is released through custom extracts that are prepared based on specifications developed with each applicant.” So it’s useful for entities that can gain access — here’s a peek at the process.
The Massachusetts APCD also charges for access to the underlying data, if you have the resources to assess it. Here’s a discussion of the conditions from the site.
“MA APCD data may only be accessed through an application process. Applications for MA APCD data must be submitted on IRBNet. Each applicant must have an IRBNet account, which can be created through the link above, and affiliate with the Massachusetts Center for Health Information and Analysis once logged in. The applicant must then complete an application form for MA APCD data and execute a Data Use Agreement, available below. All of the application documents below are also available for download in the IRBNet Document Library. For any questions about the application process, please email apcd.data@state.ma.us. Non-government applicants are subject to APCD data fees, but may be eligible for full or partial fee waivers if they meet certain criteria.
“Requests for MA APCD data are considered through a multi-layer process that reviews risks to patient privacy, research or project objectives, and the public interest. Any release of MA APCD data is screened by CHIA’s Data Privacy Committee, which includes CHIA’s subject matter experts, Chief Privacy Officer, and Chief Information Security Officer. CHIA’s Data Release Committee, composed of a variety of external experts representing carriers, providers, researchers, and consumers, provides additional scrutiny to certain applications to ensure that data release is in the public interest as defined by CHIA regulations. Please see the Data Release Flowchart and CHIA’s Privacy Program for more information about CHIA’s review process for releasing MA APCD data.”
In other words, you have to have research credentials, pass the application process and pay.
Plus, you have to speak in MA APCD IRBnet CHIA language.
Oh, and what is IRBnet? “Innovative Solutions for Compliance and Research Management,” the site says.
But Massachusetts did use the APCD data to make this tool for pricing and quality information; it’s not deeply useful, but it’s something. Also, the site says the cost information is from 2011. (Sigh.)
In some cases, the APCD has proved quite useful for big players in the marketplace to bring prices down, which should ultimately benefit consumers. But like a lot of other things in health care, individuals can’t see it.
“When Anthem Blue Cross Blue Shield became embroiled in a contract dispute with Exeter Hospital in New Hampshire in 2010, its negotiators came to the table armed with a new weapon: public data showing the hospital was one of the most expensive in the state for some services,” Julie Appleby of Kaiser Health News wrote in this piece about how APCD data can be used.
Consumer-friendly tools built from APCD data
New Hampshire has a website, nhhealthcost.org, that lists hospital prices for about 30 common procedures. While it’s interesting — the range for a common CT scan of the chest is wide, as you can see from this spreadsheet — it’s a bit misleading. This search shows the price range for a chest CT scan to be from $1,219 to $9,854. We know of an imaging center in New Hampshire, Salem Radiology, that has low cash prices, because we’ve written about them before (as has my friend ePatient Dave deBronkart, in this blog post about how he price-shopped his CT scan. The blog post includes a 2011 price list from Salem Radiology, which does not still exist on the site, showing a chest CT scan costing $260.
We also found a website for New Hampshire Open MRI, which prices MRI’s starting at $799, while the New Hampshire website shows lower-back prices from $1,270 to $4,531. So maybe the APCD doesn’t include non-hospital charges? It’s not clear, but in any case the shopping experience is diminished if lower-price options are omitted.
And, the New Hampshire website, like most others, is sometimes able to accurately compile your out-of-pocket costs if you’re insured, but sometimes not.
(From what we know, here’s some free pricing advice: Always ask what you’ll pay. These New Hampshire prices seem high to us by New York standards. Ask “How much will that cost? How much will that cost me with my insurance?” And then ask “How much would that cost if I was paying cash up front?”
Take names, and take notes. Ask the provider, ask the insurer, if there is one. And then ask again.)
Here’s another consumer-facing APCD tool, this one from Maine. I haven’t done a comparative survey on its value.
Minnesota also has a consumer-facing tool, but it’s built by MN Community Measurement, an independent, non-profit community organization.
Payers and others talk about the APCD data
Who is using them?
While just getting the legislative authority to make an APCD and then maintaining it is complicated, there’s also the question of who’s using them: policy-makers, payers, employers, health care providers, state agencies, consumers?
Private players may not be that interested in APCD data either, judging from a quick survey.
Hanny Freiwat is president and co-founder of Wellero, a new smartphone app that calls itself “a mobile retail experience for consumers of health care,” which pledges to make health care costs easy to understand by making online payments, and easing deductibles and other calculations.
Wellero doesn’t use APCD data, Freiwat said; Wellero needs near real time claims data.
“Wellero does not use APCD in its current model. We obtain claims directly from partner health plans as soon as they adjudicate. We need the data as soon as it is available for payment and consumers/people to understand the impact. I like APCD as a data source for analytics and maybe claims history but not for our current approach.”
Freiwat said the strength of the APCD lies in history and analytics, because it’s “A great way for a data analytics company to look at local, regional, and national trends.
Weaknesses?
“Timing. Today’s technology could and does deliver this data as soon as it is available vs. monthly and quarterly reporting which creates massive overhead to load and search for data.”
They’re not that useful for individuals, Freiwat agreed. He doesn’t use them: “The fact that they are state sponsored creates a challenge for nationally based solutions. Small companies like Wellero have to request access and build solutions 50 times instead of once. And the fact that no all states are participating or have voluntary opt-ins creates internal challenge for us as we try to create a standard experience in our solutions.”
Jim Delaney, chief operating officer at Advanced Medical Pricing Solutions, a health care cost containment company in Atlanta, Ga., said he too does not use APCD claims data.
“The data that I’ve seen published (mostly still aggregate) is not conducive to evaluating charges on a particular claim – and still too spotty with respect to geography,” he wrote in an email.
AMPS has contracts with multiple payers nationally and many employer groups to evaluate claims before they are paid. AMPS evaluates and makes recommendations on every claim, using physician reviewers and multiple fair reimbursement metrics. But Delaney saw more value in APCD quality metrics than pricing metrics: “Growing potential for other states to do something like Maryland and dissemination of quality measures” are among the strengths of the APCD, he said. He said he’d also looked at Pennsylvania’s new APCD file, seeing nothing of great value for AMPS in pricing, but “However, having the quality measures in one place does potentially.”
What are their weaknesses? “Emerging public policy issues; arguments about what should be required; how it should be interpreted, and permissible use,” he wrote in an email.
For individuals, he sees limited usefulness. “I’m not even sure about their usefulness today except in academia. Even there, is there any real body of work published yet?”
Are they worth the time and trouble?
Are APCD’s worth the time and trouble, given the value they deliver? That’s not clear.
Since each one is different, it’s hard to gain consensus.
The people who appropriated money for them and who work on them tend to think they are a good idea. They cost a fair amount of money, and there’s also a good bit of effort required to get legislation passed and get the APCD up and running.
People and entities that are in competition with the APCD model tend to say they’re not such a good idea. Catalyst for Payment Reform, Suzanne DelBanco’s group, mostly a coalition of large employers, is not all that enthusiastic.
The Health Care Cost Institute, a nonprofit that has as its members a number of big insurance companies, has promised to make a collection of insurance-company payment data available in early 2015; that data, the HCCI says, will help consumers. It’s not clear what that will look like.
States that haven’t set up an APCD, and why
Finally, even if the value might be seen as limited by indidviduals, and by market entities like Wellero and AMPS, in many states there is resistance to the idea of an APCD.
Washington state tried to set one up, but the legislation to make it happen was blocked, reportedly by Premera Blue Cross, the state’s biggest insurer, local news media reported.
New Jersey decided also not to do it, citing future costs.



{kind=link}